By: Robert L. Shepherd, MS, Certified Medical Illustrator, President & CEO, MediVisuals Inc.®
The fact that individuals sustaining traumatic brain injuries (TBIs) often exhibit delayed or worsening symptoms over time is well documented in medical literature (a narrated animation effectively demonstrating this process can be viewed here. Despite this fact, insurance company representatives and their attorneys frequently argue that symptoms should be immediately evident and at their most severe immediately following a traumatic event. They often claim that any delayed or worsening symptoms must be the result of an unrelated injury or disease process. They may even argue that the victim is malingering (faking the symptoms) because symptoms have developed or worsened after the initial incident. It is a challenge for attorneys representing TBI victims to overcome the jurors’ and other decision makers’ predisposition to believe that symptoms should be at their most severe immediately following a traumatic event and heal over time (like most other wounds).
Medical science has revealed that the initial stage of injuries to neurons, which results in immediate symptoms, is followed by a second stage of gradual death of neurons that progresses over a prolonged period of time and results in significant worsening of those injuries in scope and severity. The literature describes this progression and worsening of symptoms as continuing for months, years, or even for the TBI survivor’s entire lifetime. Due to this long-term progression, TBI is more accurately referred to as a “process” not an “event”.
Trauma to the head doesn’t have to be particularly severe to begin the insidious chain of events that can devastate the lives of TBI victims and their loved ones. The process begins with tears of scattered axons (long extensions of neurons that carry chemical and electrical impulses to other neurons). A partial tear of just the outer membrane may heal, or it may allow an influx of calcium ions (necessary for transfer of impulses, but very harmful if allowed to uncontrollably flow into the axon through the membrane tears).
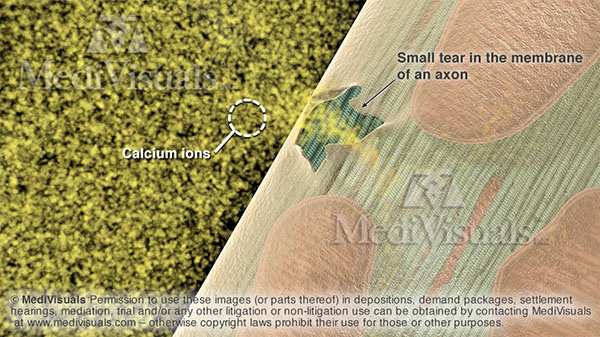
Figure 1: Calcium ions flowing uncontrollably into a small tear in the membrane of an axon.
If the influx of calcium is too great, the mitochondria within the axon begin a process of self-destruction (referred to as “apoptosis” or “suicide”). This process involves the excretion of substances from the mitochondria that break down the cell. The destructive substances also escape the cell to create small openings in the cell membranes of nearby axons, resulting in uncontrolled influx of calcium ions in the nearby axons as well.

Figure 2: Release of self-destructive substances from injured axon into surrounding fluid, where they are transported to and begin to break down nearby, healthy, functional axons.
Injured axons may partially heal and form terminal bulbs. During the destructive process and attempted healing process, the injured axons continue to receive and carry excitatory impulses. Unfortunately, as these impulses reach the injured end of the axon or the bulb, they are unable to continue across the site of disruption, and the chemical and electrical impulses are arbitrarily released. Due to a process referred to as “excitotoxicity”, these substances damage and destroy nearby axons that may have been unharmed and perfectly functional prior to this “attack”.

Figure 3: Destructive electrical and chemical impulses being discharged from a terminal bulb.
When combined with the destructive substances from the axons undergoing apoptosis (suicide), nearby axons are similarly destroyed (murdered). As they are “murdered”, they too release their internal destructive substances. Combined with the excitotoxicity of the newly injured axons, the breakdown of other nearby axons continues in an ongoing cascade.
Just as with most disease processes, different people are more susceptible to the process than others, and the speed and longevity of the destructive process can occur over weeks, months, years, or even the course of a person’s entire lifetime.

Figure 4: “Island” of spreading injured axons and terminal bulbs.
The injury process can begin in isolated pockets, or “islands”, and spread to other areas throughout the brain. These multiple, widespread lesions are often referred to as “traumatic axonal injury” or “diffuse axonal injury”. Each island of injury may involve from only a few axons, to thousands, or even tens of thousands. Because typical MRIs can only detect lesions that are about the size of the head of a pin, and tens of thousands of axons can fit through an area the size of the head of a pin, MRIs are typically interpreted as negative for TBI, even though hundreds of thousands, or even millions, of axons could be injured across the scattered areas of “traumatic axonal injury”.
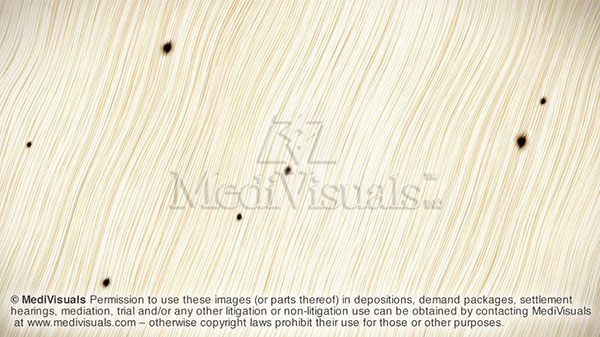
Figure 5: Multiple microscopic islands of injured axons, each consisting of hundreds, thousands, or even tens of thousands of axons – all too small to be visible on typical MRIs.
MediVisuals, Inc.® – Permission to use any image (or parts thereof) posted on this blog in depositions, demand packages, settlement hearings, mediation, trial, and/or any other litigation or non-litigation use can be obtained by contacting MediVisuals at www.medivisuals.com – otherwise copyright laws prohibit their use for those or other purposes.
