By: Robert L. Shepherd MS, Certified Medical Illustrator, President & CEO, MediVisuals Inc.®
Computer-generated 3D reconstructions from a person’s actual CT or MRI data as well as medical illustrations are powerful tools that can be used separately to demonstrate a plaintiff’s injuries. However, when used together, they complement each other in ways that greatly accentuate their individual effectiveness. For example, when an illustration is used along with digital 3D reconstruction, and the two images closely correspond with each other, the 3D reconstruction increases the perceived credibility or accuracy of an illustration. The illustration complements the 3D reconstruction by providing more realistic details of an injury or surgery through the addition of color (undetectable by scans) and other details to tissues that may also be beyond the scope of the scans to either capture or demonstrate. The heightened credibility offered by the 3D reconstructions is due to the court’s acceptance that computer generated 3D reconstructions do not alter the plaintiff’s actual scan data. Because the courts feel the images are therefore more authentic or factual than a medical illustration, the courts typically accept 3D images created from the plaintiff’s actual CT or MRI data into actual evidence (as opposed to demonstrative evidence).
When creating computer-generated 3D reconstructions from the patient’s actual 3D data, human factors and involvement are still required to eliminate tissues and artifacts in order to achieve a satisfactory end product. There are multiple 3D reconstruction softwares available, some based on FDA (Food and Drug Administration) Cleared Technology. The more sophisticated the technology, the more human involvement is required to create the end product. A technician must direct the software and make many vital decisions that will alter the appearance of that end product, such as which tissue densities will be removed to reveal underlying anatomy and pathology as well as which views will best present those findings. When the decisions are based upon sound knowledge, judgment, and experience, the images can be created in a way that helps laypeople more easily understand relevant anatomy and pathology. It is important to note that the technician is not changing the data during this process.
The primary advantage of medical illustrators creating 3D imagery (whether as a technician using the imaging software or when creating an illustration, animation, or model) is that they are able to use anatomical, medical, and biomechanical knowledge to understand and further clarify the computer-generated 3D reconstructions. This deductive reasoning is similar to the deductive reasoning required by a radiologist to interpret the images: the radiologist uses similar knowledge and reasoning to create a more accurate understanding of the imaging study in his/her own mind. A skilled medical illustrator can take this process a step further and create actual 2D or 3D imagery that clarifies the important areas in the images generated by the software alone to result in more, not less, accurate imagery by knowing which tissue densities to focus upon. The human factor, therefore, actually results in imagery that more closely and truthfully resembles the plaintiff’s real injuries.
The advantages of 3D reconstructions over illustrations are: 1) they are generally considered more precise or accurate than illustrations because human factors are felt to be removed from the interpretation of the data, and 2) they are an affordable and fast source for a digital 3D model that allows the viewer to appreciate details of the anatomy or pathology from virtually any angle. The disadvantages of 3D reconstruction are: 1) the limitations of older technology or low resolution renders result in the averaging of information that rounds off jagged or sharp edges of fractures and fills in small fractures that are otherwise visible in individual scan slices, and 2) the software, by itself, cannot differentiate between a bone joint space and fracture, and therefore cannot assign colors to differentiate between the two, unless directed by the technician. When a technician assigns color to an image created from a patient’s actual CT or MRI data, the assignment of color (for example, the assignment of red to an area to differentiate a fracture from a normal bone joint space) is no different from the decision an illustrator makes in assigning color to images. Both methods require the human to determine what is a fracture and what is not, and then assign appropriate color application to the area.
It is important to understand that at this time there are two or more generations of 3D reconstruction technology available. Older technology using less sophisticated software and lower resolution renders pose several problems as described and shown in the illustrated examples at the end of this article. Newer, more advanced technology (3D Precision DiagnosticsTM® examples and link below) is better able to differentiate between tissue densities as well as create 3D imagery with much greater detail and definition.
Another major factor determining the end product is the quality and number of original scans taken. For example, head scans are taken with slice thickness set to specific parameters. The results from scans using 1mm slices contain exponentially more data and information than results from 1cm slices. An individual 3-Tesla MRI scan contains three to four times the amount of data compared to a 1.5-Tesla MRI scan. More advanced technologies can better image details of limited data sets, but even with the best technology, if fine details of a scan need to be appreciated, it may be impossible to create adequate 3D imagery from a scan containing limited data. A technician can typically determine whether a data set is adequate in a brief period of time.
Two other factors altering 3D output are 1) the amount of time the technician spends carefully selecting tissue densities to be shown, and 2) the amount of rendering time allocated for the end product. Some companies use presets when processing typically shown imagery such as disc herniations or bulges. Therefore, one patient’s data might not show an injury as clearly as another due to the slight differences in densities not being taken into account. The second factor, allocated rendering time, means that the same data set rendered at low, mid-range, or high resolution uses vastly differing amounts of computing resources to complete the final product, such as a video. This results in a wide variation of detail shown in the final product from one resolution to another. Computing times will vary greatly between systems, but an example is that the same data taking 2 hours to render at low resolution, might take 12-24 hours at high resolution. Higher costs would be associated with more complex imagery (much more technician time upfront) and higher resolutions (tying up powerful computer resources that could be processing additional jobs in the same timeframe). A well-trained medical illustrator as the technician can advise clients as to the level of sophistication necessary to achieve a satisfactory end product for their purpose. Clients who use automated systems to place orders and upload files may be given the opportunity to “upgrade” to a more sophisticated level, if the end product desired would be substantially better and if the data provided would support a more complex render.
Examples of problems with older 3D technology and how illustrations enhance understanding:
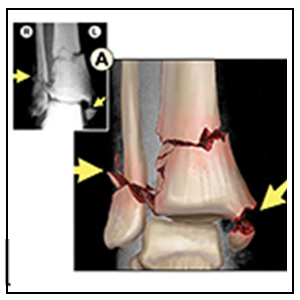
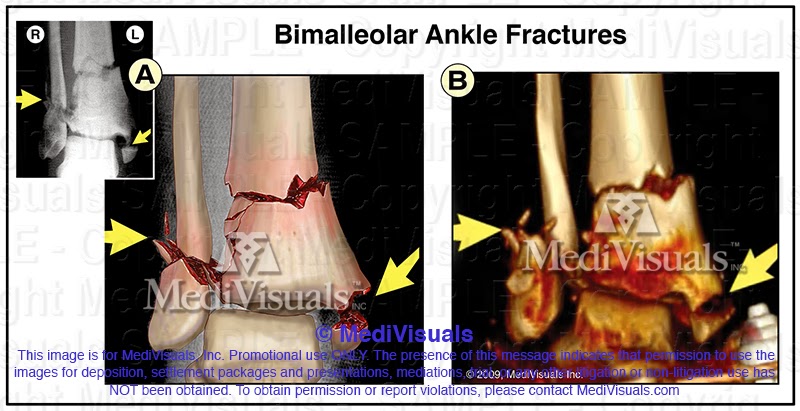
Bimalleolar Ankle Fractures:
The figure on the left is an illustration created over an AP X-ray of an ankle fracture. The figure on the right is a 3D reconstruction image from the same ankle after an external fixation device had been put in place. Note that the fractures in the 3D reconstruction are rounded off and that red artifact complicates the findings. In contrast, the illustration demonstrates the fractures with hard, sharp, or angled edges (based upon review of individual scan slices and application of deductive reasoning). Note also that some of the smaller fracture lines and fragments that only appear as bumps and lumps in the 3D reconstruction are more clearly and accurately depicted in the illustration. These fracture lines were clearly visible in the CT scan slices, but the 3D imaging software was unable to hold the detail in the 3D reconstruction.
Displaced fracture of 2nd Metatarsal:
The image on the left is an illustration of the fracture as created directly over an X-ray. The image on the right is a 3D reconstruction. Note how the 3D reconstruction rounds off the edges of the fracture, and the fracture appears very similar to one of the normal joint spaces. Note also how red artifact around the tarsal bones detracts from the actual injury. In contrast, the illustration again demonstrates the fracture with hard, sharp, angled edges. Also, as bone is known to bleed when fractured, the illustrator uses knowledge and deductive reasoning to apply red coloration to the area of the fracture and thereby represent the injury more accurately as well as further distinguishing the fracture from the various normal joint spaces.
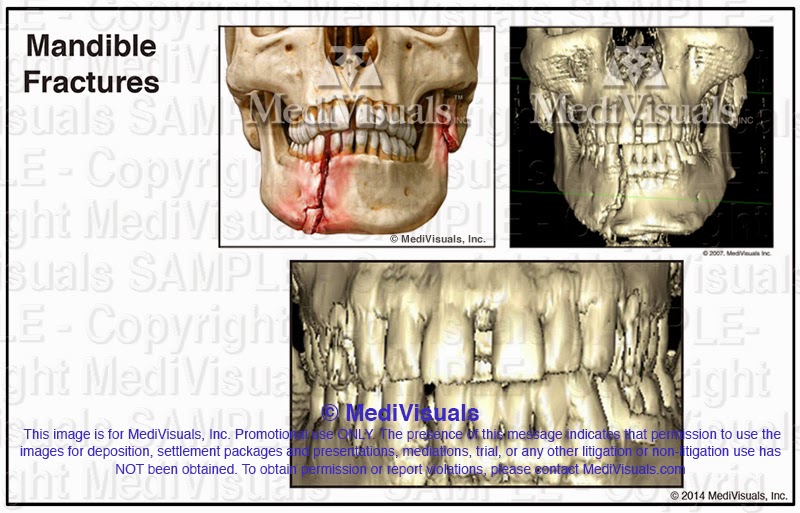
Mandible Fractures:
Note that the edges of the fracture fragments in the 3D reconstruction are again rounded. The rounded edges and lack of color make it difficult for the untrained viewer to detect the upper left fracture. By using the 3D reconstruction as well as reviewing the individual CT slices, the medical illustrator is able to create a more accurate and understandable interpretation of the injuries. Note also that the lower teeth appear to be fused in the 3D reconstruction. This is a good example of how the imaging software’s deficits do not allow it to accurately depict fine details that are evident on the individual slices. The gaps between the teeth could just as easily be small fracture lines in the bone that the 3D reconstruction failed to accurately portray, but by reviewing the individual CT scans, the illustrator can portray these details in a much more accurate representation.

Examples from 3D Precision Diagnostics®, the newest and most advanced technology available to trial lawyers at this time.
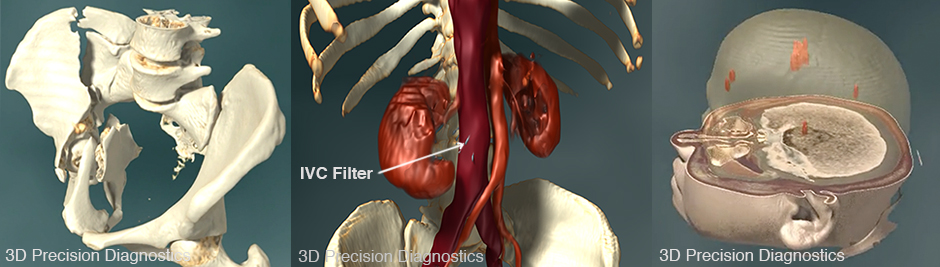
Still images taken from 3D Precision Diagnostics® videos. To view the videos, click here
Contact MediVisuals if you have any questions or would like more information on medical illustrations and/or 3D Precision Diagnostics® using Actual CT and MRI Data.
MediVisuals, Inc.® – Permission to use any image (or parts thereof) posted on this blog in depositions, demand packages, settlement hearings, mediation, trial, and/or any other litigation or non-litigation use can be obtained by contacting MediVisuals at www.medivisuals.com – otherwise copyright laws prohibit their use for those or other purposes.