
Settlement for Frivolous Defenses: Michael Maggiano
Successful Settlement for Plaintiff in Med Mal case with Frivolous Defenses
Congratulations to Michael Maggiano and his team for their success in obtaining a just settlement for their plaintiff, as well as thanks to them for the improvements in health care in New Jersey that will come about because of their efforts. Mr. Maggiano recognized multiple negligent acts by several health care providers during the care and treatment of a woman who had undergone a laparoscopic banding procedure. In spite of the fact that complicated Medical Malpractice cases are among the most difficult for deserving plaintiffs because confused jurors are known to find for the defense, the Maggiano, DiGirolamo & Lizzi team successfully took on the challenge. The case resolved for a confidential amount after two days of motion practice, four days of jury selection, and after putting on four doctors and the plaintiff. During litigation, the Maggiano team filed and won nine motions in limine. They also successfully opposed all motions by the defense. The team’s success not only helped the individual who suffered most from the negligence but also resulted in improvements in the practices and policies of the involved physicians and health care facilities.
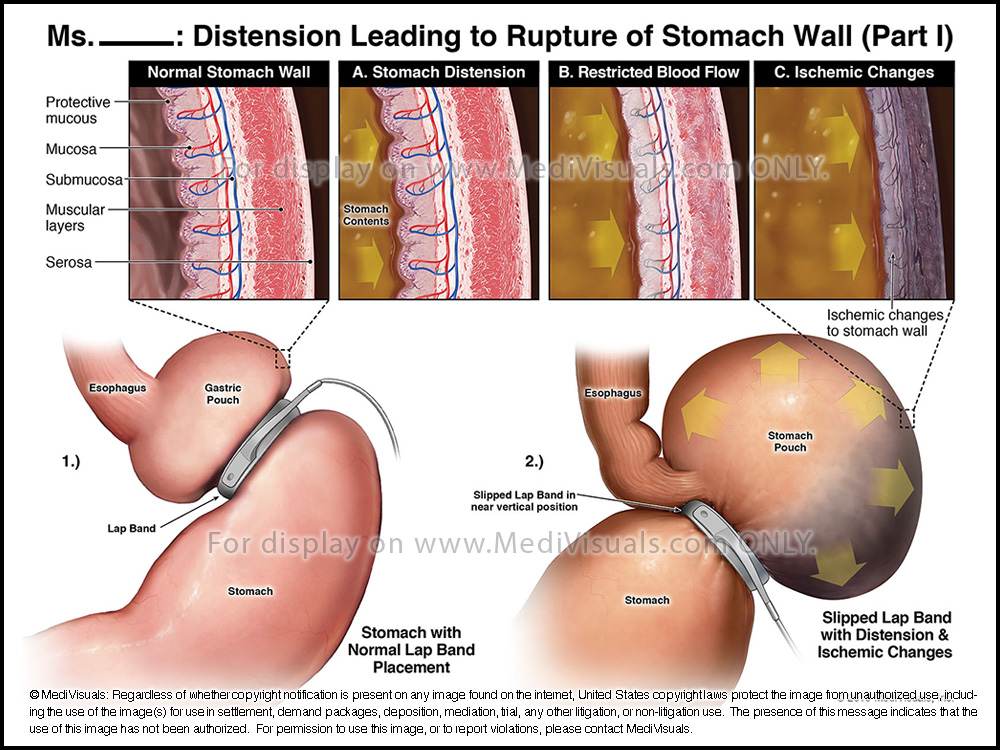
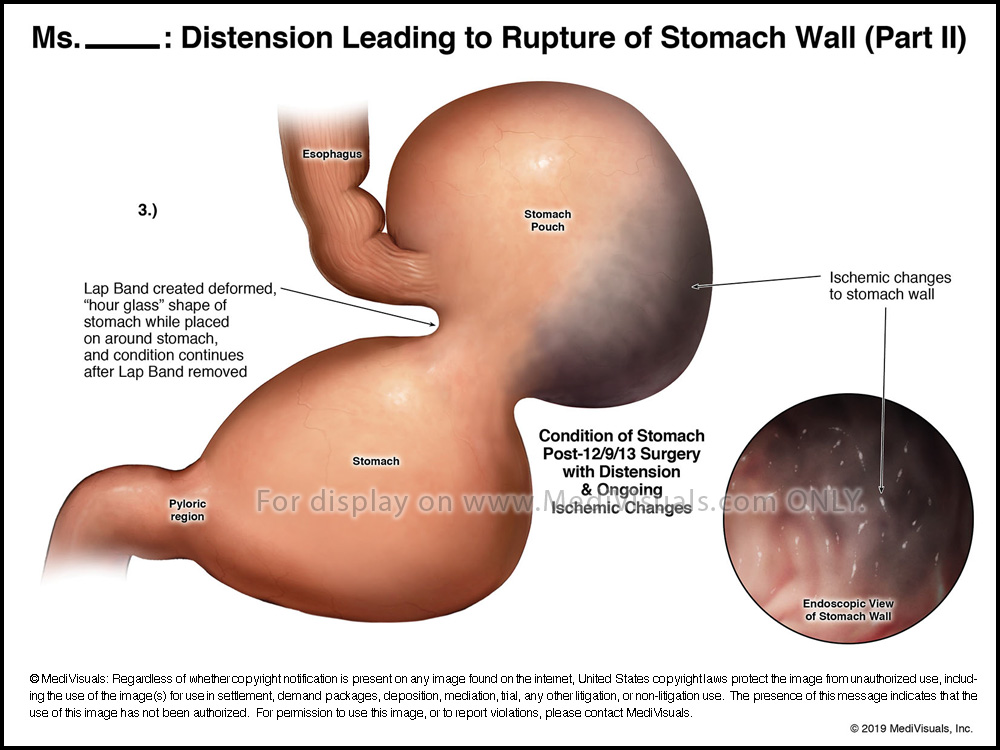
The issues of the case involved a woman who presented with symptoms of a slipped laparoscopic band several months after its placement. After continued symptoms, and after seeking help from several health care providers, the plaintiff eventually underwent an X-ray that showed the gastric band had slipped, resulting in a severely distended gastric pouch (see Figure 1). Surgery was then performed to remove the band. During the surgery, gray areas of ischemia were noted on the inner and outer stomach wall (see Figure 3B). Despite the concerning ischemic changes to the stomach, as well as other concerning findings over the next three days (elevated WBC, tachycardia, elevated temperature), the plaintiff was discharged without being told of any of these concerning findings.
Click on bottom right corner to view video in full screen
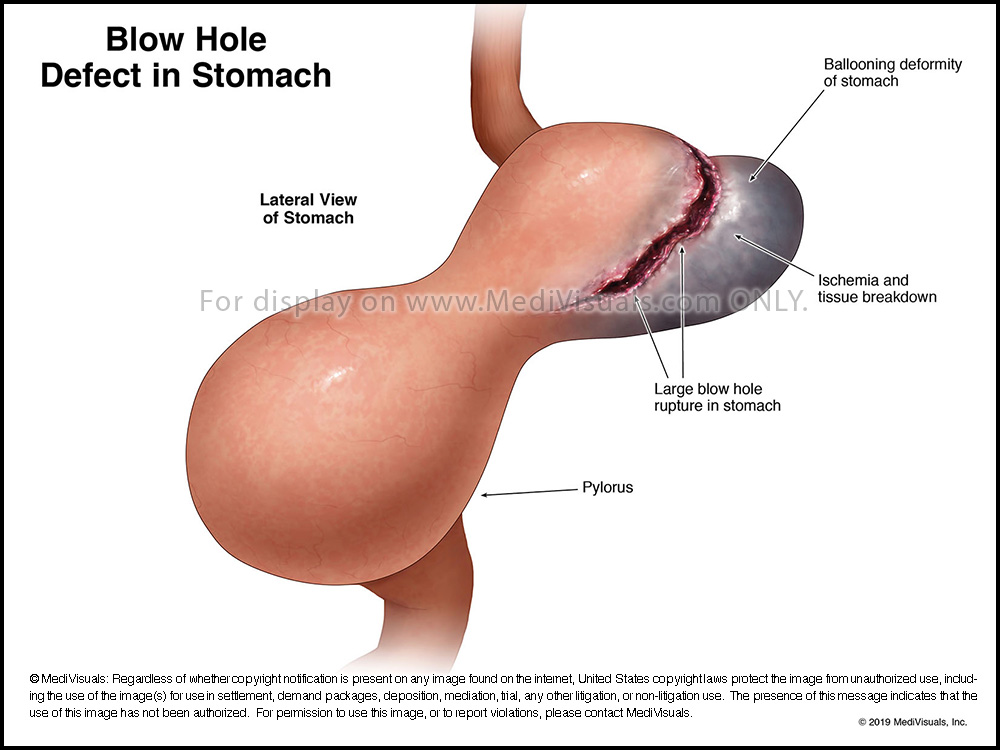
At a postop visit, the plaintiff complained of abdominal pain, to which the surgeon replied, “Of course you have pain. You just had surgery.” Over the next several weeks, the plaintiff continued to follow up with the surgeon with complaints of severe abdominal pain, but the surgeon offered no assistance. Eventually, the pain became so severe that the plaintiff was taken via ambulance to a hospital where a CT Scan was performed, revealing a gastric perforation with free fluid and air throughout the abdomen (see Figure 2). During the ensuing, emergent surgery, a large tear in the fundus of the stomach in the region of the previous ischemic areas was encountered (see Figure 7), documented, and repaired. The appearance of the abdomen suggested the perforation had been present for several weeks. Because of the delay in diagnosis, the resulting peritonitis, and sepsis; the plaintiff was severely ill for a prolonged period and underwent multiple surgical procedures.
Click on bottom right corner to view video in full screen
The surgeon who failed to adequately follow the plaintiff after the gastric band removal – who also failed to address the concerning intraop findings of stomach ischemia, the concerning postop vital signs suggestive of a bowel perforation, and the plaintiff’s repeated calls to him with complaints of abdominal pain – offered a two-fold, frivolous defense. Firstly, he denied having been informed of the concerning postop vitals. Secondly, the surgeon claimed that the plaintiff had not contacted him with multiple postop complaints of pain. The plaintiff provided phone records that proved otherwise.
The defense team presented an additional frivolous defense, claiming that the stomach perforation was not due to the slipped band and did not occur in the area of stomach ischemia, instead proposing that the perforation was the result of a typical stomach ulcer and completely unrelated to any negligence. This defense was likely created because of the rather casual and broad use of “ulcer” in a pathology report. In order to further support the “ulcer” theory, the defense argued that the plaintiff’s complications and future surgeries were the fault of the surgeon who performed the emergency surgery and discovered the perforation. The defense went on to claim that the surgeon botched the emergency repair surgery and manufactured the “fantasy” of a severe gastric rupture to cover up said “botched” repair surgery.
MediVisuals was entrusted to help develop graphics for the case. Because damages were so severe and obvious, the focus was primarily on the negligence. The graphics focused on supporting the plaintiff’s arguments, helping clarify radiographic imaging, and countering defense theories. Early on, plaintiff experts and treating physicians offered different opinions about the very crucial location and appearance of the stomach perforation that was eventually discovered during the emergent surgery and depicted in the CT taken just before the surgery. To help clarify and unify these opinions, MediVisuals enlisted the use of 3D Precision Diagnostics® CT reconstructions (see Figures 5 and 6), which offered a much clearer depiction of the stomach and abdomen anatomy than can be acquired with traditional medical facility imaging. The resulting 3D reconstructions created with the 3D Precision Diagnostics® imagery can be seen below.
Click on bottom right corner to view video in full screen
All in all, more than 30 exhibits were created from the available radiological evidence to demonstrate the evolution of the pathology, surgical repairs, and related interventions.
In New Jersey, a medical negligence case cannot settle without the surgeon’s consent to do so. Following the presentation of preliminary legal arguments, opening statements, and testimony of four treating physicians – and during the testimony of the plaintiff – the matter was settled by way of a confidentiality agreement. The plaintiff, while recognizing that no money can give her back her prior life, expressed great satisfaction with the resolution of the case in her favor and with the legal services provided by the law firm.
The Plaintiff, while maintaining confidentiality of the settlement terms, publicly expressed (on Google):
“After thirteen surgeries, multiple procedures, and over two months in the ICU, all due to the negligence of one of my doctors, I was referred to Michael Maggiano to pursue a medical malpractice case. I had never been involved in a lawsuit in my life, and from the moment I met Michael and his team at Maggiano, DiGirolamo & Lizzi, I knew I was in extremely competent hands. Michael is the best lawyer you could imagine – he is intelligent, detail oriented, extremely knowledgeable, and passionate about his work and his clients. Michael is a consummate professional, and I will forever be impressed by, and indebted to, both him and his team. The entire staff at Maggiano, DiGirolamo & Lizzi is friendly, welcoming, and do everything to make their clients comfortable. I would like to specifically thank Linda Reid and Bernadette Elbert who both went above and beyond to make my experience as comfortable as possible, from including me in all detailed correspondence to sending encouraging texts and even giving hugs when needed. Thank you so much to everyone at Maggiano, DiGirolamo & Lizzi – I highly recommend this law firm to anyone looking for a compassionate team to handle a personal injury claim.”